Ответить
|
Re: Многооскольчатый перелом плеча
Виталий Евгеньевич Казеннов 25 Сентябрь 2003, 08:11
|
По моему мнению, здесь предпочтительнее лечение скелетным вытяжением за локтевой отросток на отводящей шине. Через сутки после наложения вытяжения провести рентген-контроль и, при необходимости, закрытую ручную репозицию под наркозом. Можно будет провести исправление возможного осевого смещения через три-четыре недели, "на мягкой мозоли", при наложении торакобрахиальной повязки.
Казённов В.Е., Хабаровск
|
[
Ответить ]
|
Re: Многооскольчатый перелом плеча
Отправитель: Alexander Chelnokov 25 Сентябрь 2003, 16:29
|
Тц> По моему мнению, здесь предпочтительнее лечение скелетным вытяжением за
Тц> локтевой отросток на отводящей шине.
Удалось найти отводящую шину ЦИТО, пока пациенту нравится - по месту первой госпитализации было, видимо, накроватное вытяжение.
Тц> Через сутки после наложения вытяжения провести рентген-контроль
Тц> и, при необходимости, закрытую ручную репозицию под наркозом.
Сегодня будет остеосинтез0 вертлужной впадины, попутно и контроль положения отломков плеча можно будет сделать. Спасибо. Но про оперативную фиксацию мысли как-то не успокаиваются...
|
[
Ответить ]
|
Re: Многооскольчатый перелом плеча
Отправитель: Виталий Евгеньевич Казеннов 25 Сентябрь 2003, 16:32
|
Если я не ошибаюсь, плечо фрагментировано на шесть (!) отломков, и если "про оперативную фиксацию мысли как-то не успокаиваются..." -- металла может потребоваться очень много.
Лучевой нерв уж очень в зоне доступа.
Если бы это была моя рука, я бы попросил шину ЦИТО. А потом, если осевое положение более или менее удалось бы откоррегировать -- укороченную повязку типа Сармиенто-Охотского.
|
[
Ответить ]
|
|
Re: Многооскольчатый перелом плеча
Andrea Salvi 25 Сентябрь 2003, 08:12
|
Dear colleague,
what a terrible fracture !!!!
I suggest an extensive approach starting with a shoulder approach (i.e. a Deltoid-Pectoral one) passing on the lateral face of the arm and arriving to the elbow with a Fiolle-Delmas approach.
This elongated approach permits to evaluate all the humerus unforgetting any detail.
So it is possible to put cerclages and a long plate according to the needs of the moment.
Best regards,
Andrea Salvi - MD
Spedali Civili di Brescia
2' Divisione di Ortopedia e Traumatologia
Clinica Ortopedica dell'Universita (Direttore : Prof. U.E. Pazzaglia)
25100 BRESCIA - ITALY
|
[
Ответить ]
|
Re: Многооскольчатый перелом плеча
Bryan Neal 25 Сентябрь 2003, 08:57
|
That is the worst humerus I have seen.
I think I would treat it nonoperative.
There is a humerus rod with a blade plate that could be secured into the humeral head. Synthes make it. I have not used it.
Sincerely and respectively,
M. Bryan Neal, MD
Arlington Orthopedics and Hand Surgery Specialists, Ltd.
1100 W. Central Road, Suite 304
Arlington Heights, Illinois 60005
(phone) 847-394-5650
(fax) 847-394-5699
(email) AOBoneDoc@aol.com
|
[
Ответить ]
|
Re: Многооскольчатый перелом плеча
GOBINDER SINGH 25 Сентябрь 2003, 08:58
|
This IS a terrible fracture, are the neuro-vascular bundles OK? With respect, Dr Salvi's approach is "classical AO thinking", from a country where the Ilizarov technique was first used outside Siberia! Cattani, Cataneo, etc, must be most upset that their teaching is being forgotten already...Even the AO giants would not do the classical approach here, I think.
With an open, comminuted fracture of the humerus, the option chosen must respect the soft tissues, or an infected non-union will be the result. I would chose either a hybrid Ilizarov-type fixation, with half-pins proximally and wires distally, or a locked IM nail.
Gobinder
___________________________
GOBINDER SINGH, FRCS
Consultant Orthopaedic Surgeon
Pantai Medical Centre
59100 Kuala Lumpur
Malaysia
|
[
Ответить ]
|
Re:Многооскольчатый перелом плеча
Отправитель: Andrea Salvi 27 Сентябрь 2003, 01:33
|
Dear Dr Gobinder,
of course this is a terrible fracture (we both said the same).
Because our colleague (who proposed the case) didn't told anything about neurovascular bundle, focusing our attention to the kind of fracture I
thought it was OK. Of course Ilizarov is a very good and reliable device, but in the proposed case, in my opinion, is of the utmost importance to investigate all the bone fragments, and, so on, to investigate also the neurovascular bundle if it is damaged.
A locked nail would be a hazardous choice, because of the multifragmentary fracture.
And, don't be afraid: Catagni (not Catani) and Cattaneo (not Cataneo) Ilizarov teaching will never be forgotten: the results using Ilizarov
devices are successfully. Suggesting an extensive approach, I have just given my opinion.
Sincerely,
Andrea Salvi - MD
Spedali Civili di Brescia
UniversitЮ degli Studi di Brescia
Clinica Ortopedica dell'UniveristЮ (Direttore : Prof. U.E. Pazzaglia)
2' Divisione di Ortopedia e Traumatologia
Address : P.le Spedali Civili , 1
25100 BRESCIA - ITALY
|
[
Ответить ]
|
|
Re: Многооскольчатый перелом плеча
Enes M. Kanlic 25 Сентябрь 2003, 16:28
|
Although we can not see exactly the head piece, and assuming that there are not signs of infection, my suggestion would be to do some type of "bridging" procedure : implant fixation in head piece and distal main fragment, and the rest to be left on its soft tissue attachments (living bone graft).
I just did this attached case, using 90 degrees angled blade plate, and this would be my preference in all similar cases.
Two days ago, I had to plate TWO humeral NONUNIONS after intramedullary nailing. Just to remove them from proximal end, significant damage had to be done to the rotator cuff. My belief is (and supported by the most of recent literature) is that the plating is a better option for humeral fractures.
Of course, external fixation could be an option, especially if we are worried about infection - but you do not need any advices in that regard.
Good luck and send us your postoperative images, please. Sincerely,
Enes M. Kanlic, M.D., Ph.D.
Associate Professor
Ortho Department at TTUHSC
El Paso, Texas
|
[
Ответить ]
|
Re: Многооскольчатый перелом плеча
Отправитель: Alexander Chelnokov 05 Октябрь 2003, 13:41
|
EKTE> rest to be left on its soft tissue attachments (living bone graft).
EKTE> I just did this attached case, using 90 degrees angled blade plate, and
EKTE> this would be my preference in all similar cases.
We don't even have so long plates in stock...
EKTE> Two days ago, I had to plate TWO humeral NONUNIONS after intramedullary
EKTE> nailing.
:-)) Yesterday i nailed a humeral nonunion after plating failure. IMHO it takes some special measures to provide nonunion after closed nailing
of the humerus...
EKTE> done to the rotator cuff. My belief is (and supported by the most of recent
EKTE> literature) is that the plating is a better option for humeral fractures.
We now use plates only for fractures of the humerus with articular involvment.
EKTE> Of course, external fixation could be an option, especially if we are
EKTE> worried about infection - but you do not need any advices in that regard.
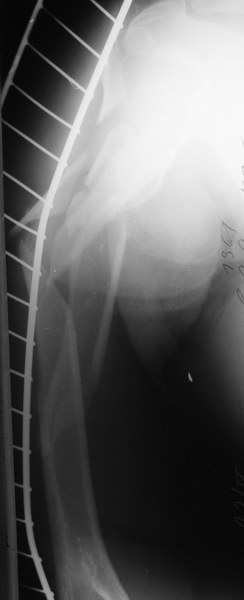
Well, to date he is still on abduction splint with traction applied to a wire placed through the olecranon. Images attached. The acetabulum
was ORIFed. The humerus is still discussing...
|
[
Ответить ]
|
Re: Многооскольчатый перелом плеча
Отправитель: James B. Carr 05 Октябрь 2003, 13:48
|
The views you now show demonstrate an extra articular fracture with good alignment on the AP, and some displacement on the lateral.
This should be able to be managed with adjustment of the traction.
Ilizarov is probably the best fixation if you decide to do so. However, it will heal with nonoperative treatment, with painless, reasonable
function. Even if it does not heal primarily, the pieces will heal enough to become a single level problem, readily solved with compression
plating. Jim Carr
James B. Carr, MD
Palmetto Health Orthopedics
5 Medical Park Drive
2 West
|
[
Ответить ]
|
|
Re: Многооскольчатый перелом плеча
James Carr 25 Сентябрь 2003, 17:49
|
Is the humeral head involved? If not, I would initially place in coaptation splint, and rex-ray. It may line up, in which case nonoperative treatment can be considered. Other options include locking nail, long bridge plate. IM nail prefeered to those, but I am not sure we improve the natural history by operative treatment. Stiffness is expected, and in my experience, related to the original injury more than
other factors.
|
[
Ответить ]
|
Re: Многооскольчатый перелом плеча
Отправитель: Bill Burman 26 Сентябрь 2003, 16:52
|
>nonoperative treatment can be considered.
see example of nonoperative rx of an open, comminuted humerus shaft fx
from Gus Sarmiento's OTA Basic Fx Course Lecture
http://www.hwbf.org/ota/bfc/sarm2/ft012.html
Bill Burman, MD
HWB Foundation
http://www.hwbf.org
|
[
Ответить ]
|
|
Re: Многооскольчатый перелом плеча
DR Cherian Kovoor 26 Сентябрь 2003, 16:54
|
Considering that it is a shattered fracture and there is nothing to gained by open reduction and fixation especially encirclage wiring why dont you immobilise in POP U slab. Most of the fragments will unite and any non union [ which will be in the shaft ] can be tackled later Encirclage wiring and extensive exposure in my opinion only would devascualrise the bone fragments.
DR CHERIAN KOVOOR
KOCHI
INDIA
|
[
Ответить ]
|
Re: Многооскольчатый перелом плеча
Peter Romchuk 27 Сентябрь 2003, 01:29
|
Closed approximation of fragments under moderate traction by hand, then tube-like (Sarmiento type) plaster cast with forearm free and suspended on a sling. It looks somewhat like U-type cast for ankle fractures. Early (range 20") movements with forearm.
I hadn't believed in this method, until tried it on one pt; results were above all expectations.
Interesting, that alignment on X-ray pics of, say 1 month duration will be looking better than on early ones. The main principle to follow is free suspension of the humerus under its own weight without axial load.
Sleeping in semi-supine position. In 3 months you'll get united humerus with mobile shoulder and elbow. Main arguments against ORIF:
1. the rate of comminution, revealed on operation, may much exceed that on x-pics.
2. presenting hematoma is a major contributor to the healing; it will inevitably be lost during open reduction and lengthen healing time despite possible good post/op. pictures.
Regards,
Peter Romchuk, orthopedic surgeon,
Central City Hospital, Rivne, Ukraine
|
[
Ответить ]
|
Re: Многооскольчатый перелом плеча
Отправитель: Len Funk 27 Сентябрь 2003, 01:31
|
Do you have any pictures of this technique to show us?
Len
Lennard Funk
Consultant Shoulder & Upper Limb Surgeon
Honorary Clinical Lecturer
www.sportsmedclinic.com
www.shoulderdoc.co.uk
www.orthoteers.co.uk
|
[
Ответить ]
|
Re: Многооскольчатый перелом плеча
Отправитель: Rajesh 27 Сентябрь 2003, 01:39
|
Good technique.
One problem I have occassionally seen in cast treatment(not this technique) of humerus #s is the risk of a sharp spike of bone piercing through the skin at some stage or other and going unnoticed until cast is taken off. Any experience of this and how would you try to avoid such a problem? (serial ultrasound ??)
thanks
rajesh
Dr.K.R.Rajesh,MS,DipNB,FRCS,FRCS(Orth)
Consultant Orthopaedic surgeon
Lords Hospital & Cosmopolitan Hospital
Trivandrum
India.
|
[
Ответить ]
|
|
Re: Многооскольчатый перелом плеча
Tom DeCoster 27 Сентябрь 2003, 01:38
|
It is very difficult to comment meaningfully without knowing whether or not the proximal humerus is involved and to what extent. There must be some sort of radiograph that shows the proximal humerus better.
Tom DeCoster
|
[
Ответить ]
|
Re: Многооскольчатый перелом плеча
Evgueny Tchekashkine 27 Сентябрь 2003, 01:47
|
Согласен с Вашей *неуспокоенностью* мысли по поводу оперативной фиксации.
Но для окончательного планирования хирургии хотелось бы видеть самою головку плеча, насколько фрагментирован перелом. Если только отрыв большого
бугорка, то предпочтительна его фиксация либо спицами и проволочной петлей либо спонгиозным шурупом , а потом ВКДО. Лигаментотаксис позволит восстановить длину и осевую ориентацию отломков, подвижность больного. Если головка фрагментирована (3-4 фрагментный перелом) когда фиксация их невозможна, то Колдуэл повязка или вытяжение на торакобрахиальной шине могут быть применены, хотя следует признать, что вероятность контрактуры плечевого сустава при консервативном лечении выше.
Всего доброго,
До скорой встречи на московской земле,
Евгений Чекашкин
|
[
Ответить ]
|
Re: Многооскольчатый перелом плеча
Святенко Владимир 28 Сентябрь 2003, 04:56
|
Если состояние кожного покрова и раны, а так же общее состояние больного позволяют произвести оперативное лечение, на мой взгляд предпочтительней произвести остеосинтез длинной реконструктивной пластиной ( как при переломах костей таза ). Консервативное лечение, в частности - вытяжение или повязка по Колдвеллу - не из оптимальных, так как надо учитывать возраст больного ( в плане результатов и возможных сроков консерв. лечения , а так же возможную значительную дистракцию фрагментов при лечении по Колдвеллу ). При операции не нужно стремиться к идеальной репозиции фрагментов. Хотя очень желательно - вторую проекцию и качественный снимок проксимального отдела!
Успехов, Владимир.
|
[
Ответить ]
|
Re: Многооскольчатый перелом плеча
Смиров Алексей 08 Октябрь 2003, 22:12
|
Уж простите меня что так вот влез на сайт! Но никак не могу достучатся до Рункова по почте. Во первых: Лёха, ты прочитал что там я накорябал? Во вторых есть несколько тазов которых хотелось бы обсудить!
|
[
Ответить ]
|
Re: Многооскольчатый перелом плеча
Смиров Алексей 08 Октябрь 2003, 22:22
|
Ну и зачем же оперировать? Тем более что вы не советуеете добиваться адекватной репозиции. И уж совсем не стоит проводить аналогии с тазом! Лично мое мнение: не надо лезть открыто,ведь всегда возникаеает самый главный вопрос - что лучше для больного? В этом случае консервативное лечение приведет к таким же результатам что и оператиное. Так стоит ли игра свеч?
|
[
Ответить ]
|
( Ответить )
|
|